
Synthesis: noun, plural syn·the·ses [sin-thuh-seez] .
- the combining of the constituent elements of separate material or abstract entities into a single or unified entity (opposed to analysis,) the separating of any material or abstract entity into its constituent elements.
- a complex whole formed by combining [disparate data elements].
If nothing else, I spend most of my day reading a LOT of online posts. Perhaps too much. But I want to throw this out from my background (in my now distant past) of molecular biology and as a software engineer that has ALWAYS kept a systems approach as it relates to our current medical crisis. I make NO claim of being a doctor, a currently practicing biologist nor researcher (although I do have a degree in Bio). And the following may be WAY off base, but sometimes I can’t stop thinking.
So, what’s my “synthesis” that could/might/be silliness?
Data Points: From my earlier post:
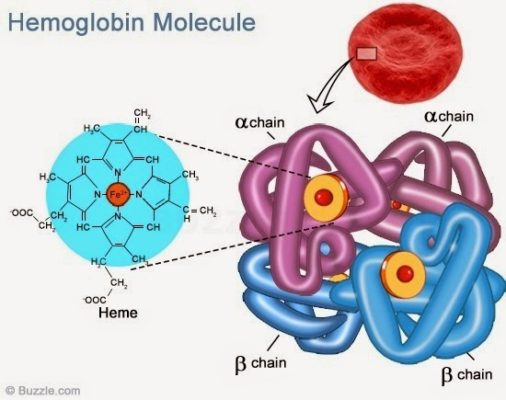
- Steve’s post pointing to the Medium post talking about the biochemistry of hemoglobin and COVID-19
- Mike’s addition (in our Grokster SLACK workspace) of the more scientific paper on how the iron ion is being stripped out of the heme molecule by COVID-19
- A layman’s background video on COVID-19 (a quick background review for me on a number of mechanisms I had long forgotten)
Add-in:
4. What my Mass General Hospital nurse sister-in-law working on COVID floors has told me and this video she sent to me – an NYC doc saying that this is not a pneumonia problem in the lungs but a symptomatic presentation of High Altitude Sickness medically known as hypoxia body-wide – but WHY? Sometimes this is a VERY rapid onset, unlike H.A.S.
5. Various sites I’ve been reading the last few days talking about the unknown reasoning as to why there are low blood and organ oxygen levels in patients even when the lungs are still “untouched” and clear.
Observations:
- #4 and #5 establish low oxygen levels.
- #3 quickly goes over immune defense mechanisms that can explain the “shattered glass” of compromised lungs after giving some amount of background. It mentions hypoxia as well but puts the burden of low oxygen observations of a compromised O2/CO2 gas exchange in the lung’s aveola sac that is suffering from severe disruption from immune cascade.
- But the low O2 levels are seen without the compromised lungs.
- H.A.S is plausable when climbing mountains – these patients are at sea level (at least in Boston). Thus, the reason isn’t that there isn’t enough oxygen in the surrounding atmosphere.
Connect the Dots: It seems that there are two fault points / root problems:
- CO2/O2 transfer across the aveola membrane is an immune backlash that is oxidative overload in the lungs.
- O2 delivery within the body.
Summary:
- The doc is right AND that scientific paper is right.
- This is a biochemistry failure in the red blood cell heme molecules caused by COVID-19 that results in low O2 levels all over.
- With no iron in the heme, the red blood cells are not transporting O2 from and CO2 back to the lungs.
- Immune reactions stop the gas exchange in the lungs as a result of the free Fe ion.
Fine and dandy, sorta. What does that lead me to?
Hypothesis: replace the damaged red blood cells with compromised / failed hemoglobin with massive red blood cells that are COVID-19 free.
Expected Results – depending on the patient’s current viral load and health:
- Expectation 1: the patient will recover for X amount of time (depending on the viral load, will the transfused blood become infected faster than the body’s immune system can kill the virus?) but may still not benefit long term (e.g., too ill in the beginning and multiple failures too far along to be of benefit).
- Expectation 2: the infusion of X amount of red blood cells will provide sufficient time for the immune system to lower the viral load assuming that the transfusion is administered in time to keep organs from failing.
- Expectation 3: a complete waste of time and red blood cells.
Again, the root cause is the COVID-19 attack on the red blood cells. Supplying undamaged red blood cells should restore more normal blood and organ O2 levels. A secondary technique would be needed to mitigate the issue of the now free iron ion’s oxidative effects (eg., lung function and health).
I told my sis-in-law (“SIL”) this – if the heme molecule is already destroyed, instead of concentrating on the lungs (looking bad from immune response cascades from over oxidation from that iron ion instead of pneumonia), stop with the ventilators. Her idea of using hyperbaric chambers (although I’ve seen that idea out on the ‘Net as well) will be of minimal help – O2 osmosis won’t be of much value when the primary mechanism is all but defunct.
I proposed this to my SIL nurse to “float” to someone else – either to reject out of hand or as something to stir yet more ideas. Well, what do you have to lose in trying this? The question is to find someone who is sick enough in that there is some hope of recovery and not someone who is too far gone to be of use as, to be blunt, as an experimental subject.
Variations of the above might be worthwhile to try.
At worst, this is just mumbling. Better is that someone else sees this and it starts another chain reaction of ideas in others. Or best, it may actually work?